
Buh bye RUG IV, hello RCS-1?
In a recently released Advanced Notice of Proposed Rulemaking(ANPRM),CMS gives us our first glimpse into a potentially new resident classification system that would replace the RUG-IV classification system to determine SNF payments. This new system, cleverly named, the Resident Classification System (RCS-1) may be slated to go into effect in FY2019. CMS released the ANPM to solicit comments and concerns related to this new system.
CMS explains the goals in developing an alternative case mix classification system are to:
- Address concerns about current incentives for SNFs to deliver therapy to beneficiaries based on financial considerations, rather than clinical characteristics and identified clinical needs;
- To maintain simplicity by limiting the number and types of elements used to determine the case mix classification as well as the number and types of assessments needed throughout a beneficiaries Medicare Part A stay.
Introduction to RCS-1
In the current RUG-IV case mix classification system, the RUG rate is determined based on 3 primary components: Therapy component, Nursing Component which are both case mix adjusted; and then the non-case mix adjusted component.
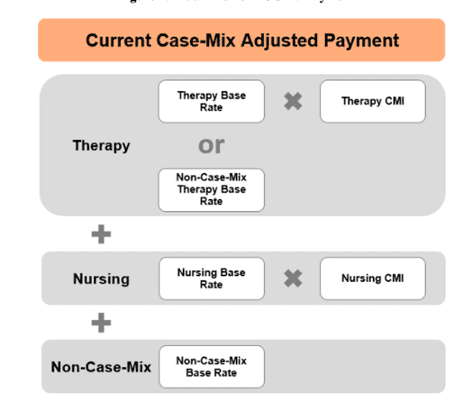
Source: Acumen SNF Payment Models Research Technical Report, April 2017
Under the new RCS-1 classification system, the payment will be determined on 5 different components: PT and OT, SLP, Nursing, Non-therapy ancillaries which will all be case mix adjusted based on resident characteristics. The final component is the non-case mix base rate which is not case-mix adjusted.
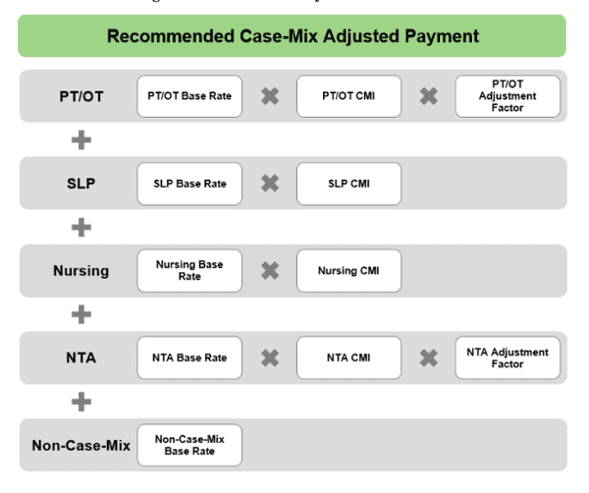
Source: Acumen SNF Payment Models Research Technical Report, April 2017
Each of the case mix adjusted components will be determined based off specific resident clinical characteristics that will be determined by the coding of specific MDS items. For the PT and OT and the SLP components, the number of therapy days and minutes will no longer be a deciding factor.
The PT/OT component will be classified based on 1) the clinical reason for the SNF stay, 2) the resident’s functional status (ADL score) and 3) the resident’s cognitive status. Once these 3 variables are determined, the resident will be classified into one of 30 PT/OT case-mix groups.
The SLP component would be determined by 1) the clinical reason for the SNF stay, 2) the presence of a swallowing disorder or mechanically-altered diet and 3) the presence of an SLP-related comorbidity or cognitive impairment. Once these variables are determined, the resident would then be classified into one of 18 SLP case mix groups.
The nursing component would mirror the current 43 nursing RUGs currently in use in the RUG-IV system (Extensive Services, Special Care High, Special Care Low, Clinically Complex, Impaired Cognition/Behavior and Reduced Physical functioning.
The non-therapy ancillary (NTA) component would also be derived from resident specific clinical characteristics. Currently, costs (labs, medications, medical supplies, etc) related to NTA’s are accounted for in the nursing component of the case-mix score. Under the RCS-1 system, NTAs would have a separate and distinct NTA component. The NTA component would be derived from a 6 different case mix groups that would be determined based on a NTA score. The NTA score would be based off specific clinical items coded on the MDS.
Summary of RCS-1 Case Mix Components
| Component | Groups |
Clinical Variables |
Other |
| PT/OT | 30 |
|
Per-diem adjustment. |
| SLP | 18 |
|
|
| Nursing | 43 |
|
|
| NTA | 6 |
|
Per-diem adjustment. |
MDS Assessment Schedule
Another significant change, if implemented, will be related to the MDS assessment requirements under the new program. To address industry concerns related to the frequency and number of PPS assessments as well as the increasing complexity around PPS assessment rules, CMS is proposing to significantly reduce the number of assessments needed under the new RCS-1 system.
CMS is proposing to require two assessments for payment classification and will also continue to require the completion of the SNF PPS Discharge assessment, for a total of only 3 assessments. The OBRA assessments are not impacted by this new payment classification system and will still be required.
Each resident will have the 5-day PPS assessment required to be completed. This will determine the initial resident classification which will be in effect for the entire Medicare stay unless a SCSA is warranted.
Proposed Assessment Schedule under RCS-1
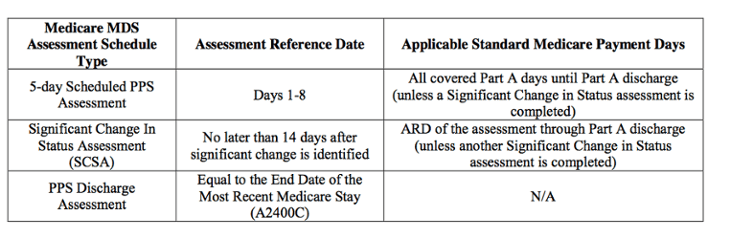 Source: CMS -1686-ANPRM, April 2017
Source: CMS -1686-ANPRM, April 2017
The new RCS-1 classification system also addresses those instances in which a person may be discharged and readmitted to the SNF. CMS is considering implementing an “interrupted stay policy”. This policy would define any readmission to the same SNF within 3 days of discharge and would be considered a continuation of the previous stay. The classification the resident was in prior to discharge would continue.
If the resident is readmitted to the same SNF more than 3 calendar days after discharge, or if they are readmitted to a different SNF, then a new stay would begin and necessitate the completion of a new 5-day assessment (interrupted stay).
Payment Adjustments During Medicare Stay
Under the new proposed assessment schedule, it would most likely be possible for a resident to remain in the same classification for the entire Medicare Part A stay. This however, does not mean that the SNF would be paid at the same per diem rate for the entire SNF stay.
CMS proposes to include per diem rate adjustments that would decrease the per diem rate periodically throughout the SNF Part A stay. CMS proposes both a PT/OT adjustment factor as well as an NTA adjustment factor. CMS contends that this will appropriately adjust payments for decreased resources utilized as a Medicare stay progresses.
Summary
As you can see, the new RCS-1 payment system, if implemented will require a strategic shift in operations as well as a concentrated focus on MDS accuracy to ensure each of the case-mix components are accurately determined.
No time has yet been determined for implementation and much detail is yet to be shared. But know change is coming, and it is not far away.
For more in-depth detail, you can review the 109 page ANPRM here. SNF providers and other stakeholders may submit comments through June 26th, 2017.
Relias Learning partners with skilled-nursing organizations to provide regulatory compliance training. Learn more.